microstrabismus, stereo vision
 Comments(2)
Comments(2)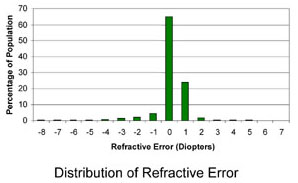 According to this distribution, the mild amount of hyperopia (far-sightedness) I have in both eyes is in statistically acceptable ranges, and is easily corrected optically. Even without correction, this amount of hyperopia — unlike myopia — is such that I could and did get away with normal accommodation. After a visit to a very thorough ophthalmologist, though, I found out that refractive error was the least interesting thing about my vision, and as a result I finally have answers to everything that I had wondered about for years. For example, now I know why it was more difficult for me to see those Magic Eye images.
According to this distribution, the mild amount of hyperopia (far-sightedness) I have in both eyes is in statistically acceptable ranges, and is easily corrected optically. Even without correction, this amount of hyperopia — unlike myopia — is such that I could and did get away with normal accommodation. After a visit to a very thorough ophthalmologist, though, I found out that refractive error was the least interesting thing about my vision, and as a result I finally have answers to everything that I had wondered about for years. For example, now I know why it was more difficult for me to see those Magic Eye images.
When I was younger, one of my eyes was much weaker than the other, and this probably began as a purely refractive disparity. But even with the help of glasses of the right optical power, the weaker eye still could not see as clearly as the stronger one. This was a condition known as amblyopia, where the vision system does not develop the neurological processing capability to deal with a high-resolution image from the weaker eye, because a high-resolution image was not available! The usual solution was to patch the stronger eye for extended periods of time (years) and force visual input entirely through the (optically corrected) weaker eye, in order to retrain the brain. This I did and it worked fairly well, but to this day, visual perception through the weaker and stronger eyes, though they are only 0.25 diopters apart in refractive error, still differ in contrast registration and edge detection. It’s hard to describe what I see on paper, but vision through the amblyopic eye isn’t blurry or fuzzy, just… less perceptive; everything makes a lesser impression and it takes longer to process what is seen.
 Be as it may, there were apparently further issues. Just as hyperopia can be corrected with a converging lens, so can the natural lens of the eye be made more converging with accommodation. I must have done this a lot because it is purely instinctive. However, the extra accommodation to bring a target object into focus tends to couple to the accommodation reflex, which also makes eyes direct toward a point closer than where the object actually is, meaning the eyes are not both looking directly at an object. This is esotropia (cross-eyed), and in small amounts where it is not noticeable, it is called microstrabismus. I took some measurements of myself looking at a single point while covering and unconvering each eye. It turns out the dominant eye (which for obvious reasons is the stronger eye) looks directly at the point at all times, while the non-dominant eye (the amblyopic eye) only looks at the point when the other eye is covered, but flicks inward just a tiny bit as soon as the latter is uncovered. This means that during binocular vision, the amblyopic eye is not even looking directly at the target object, so the image into that eye falls askew of the highest-resolution fovea of central vision, and the brain consistently gets a poorer, displaced image from it. This affects stereo vision in subtle ways.
Be as it may, there were apparently further issues. Just as hyperopia can be corrected with a converging lens, so can the natural lens of the eye be made more converging with accommodation. I must have done this a lot because it is purely instinctive. However, the extra accommodation to bring a target object into focus tends to couple to the accommodation reflex, which also makes eyes direct toward a point closer than where the object actually is, meaning the eyes are not both looking directly at an object. This is esotropia (cross-eyed), and in small amounts where it is not noticeable, it is called microstrabismus. I took some measurements of myself looking at a single point while covering and unconvering each eye. It turns out the dominant eye (which for obvious reasons is the stronger eye) looks directly at the point at all times, while the non-dominant eye (the amblyopic eye) only looks at the point when the other eye is covered, but flicks inward just a tiny bit as soon as the latter is uncovered. This means that during binocular vision, the amblyopic eye is not even looking directly at the target object, so the image into that eye falls askew of the highest-resolution fovea of central vision, and the brain consistently gets a poorer, displaced image from it. This affects stereo vision in subtle ways.
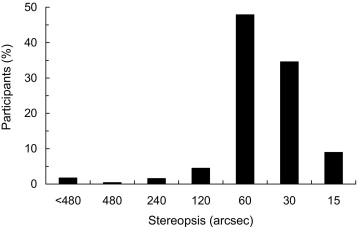 In binocular vision, when the images from the two eyes are displaced slightly, the brain does fusion and a single stereo image is perceived. When the images are displaced too far apart, the brain either sees double or perceptually suppresses one of the images (usually the one from the non-dominant eye). With microstrabismus, even looking at infinity which should normally produce identical images in both eyes, the brain is receiving doubled images, so the brain learns to completely suppress one of the images if displacement is not large enough. This results in perceptual blindness in the amblyopic eye and monocular vision whenever the stereopsis angle is small. It can be measured. Normal stereo vision goes down to about 20-30 arcseconds. My stereo vision reaches about 60 arcseconds, good enough to not be noticeable except when presented challenging scenarios like stereopsis tests or the initial effort to see the Magic Eye. But it also means that I have no depth perception once objects are about half a room away, unless I have other cues, like on this test where I know what to look for and can concentrate on undoing the suppression.
In binocular vision, when the images from the two eyes are displaced slightly, the brain does fusion and a single stereo image is perceived. When the images are displaced too far apart, the brain either sees double or perceptually suppresses one of the images (usually the one from the non-dominant eye). With microstrabismus, even looking at infinity which should normally produce identical images in both eyes, the brain is receiving doubled images, so the brain learns to completely suppress one of the images if displacement is not large enough. This results in perceptual blindness in the amblyopic eye and monocular vision whenever the stereopsis angle is small. It can be measured. Normal stereo vision goes down to about 20-30 arcseconds. My stereo vision reaches about 60 arcseconds, good enough to not be noticeable except when presented challenging scenarios like stereopsis tests or the initial effort to see the Magic Eye. But it also means that I have no depth perception once objects are about half a room away, unless I have other cues, like on this test where I know what to look for and can concentrate on undoing the suppression.
This amount of stereo-acuity is not really an outlier, but I know my limits now. As the ophthalmologist says, as long as I don’t plan on being an “elite athlete,” I am okay.
P.S.: This article on psychovisual effects on acuity (pdf) is interesting, too.

Nice post ! Subnormal stereo-acuity is also a deterrent to some professions such as airplane pilots, surgeons and like you mentioned “elite athelete.” Apart from this, such eyes are essentially normal and can lead a normal life.
its an awesome article sharing with us. eye is important in our body.thank you